Therapy aids worksheets are structured paper or digital tools that guide clients through specific therapeutic exercises, typically aligned with evidence-based treatment modalities like CBT, DBT, ACT, or trauma-focused interventions. They’re not busywork—though I’ve definitely seen practitioners use them that way, which honestly drives me up the wall—they’re scaffolding for between-session practice and skill consolidation.
What Makes a Worksheet Evidence-Based
Evidence-based doesn’t just mean “a therapist made it.” It means the worksheet operationalizes techniques from treatments that have empirical support for specific conditions or symptoms. A CBT thought record, for instance, is evidence-based because it directly applies cognitive restructuring principles that have decades of research backing for depression and anxiety disorders. A generic “gratitude journal” prompt isn’t necessarily evidence-based unless it’s structured around specific gratitude interventions tested in controlled studies.
I remember back in 2019, a newly licensed therapist in a supervision group I was in kept handing out Pinterest-style worksheets with pastel watercolor borders that said things like “list three things that make you smile.” When we asked what treatment model she was working from, she looked confused. That’s the problem—worksheets need theoretical grounding. You can’t just throw paper at problems.
The distinction matters because insurance companies, licensing boards, and increasingly clients themselves want to know that interventions have research support. If you’re documenting that you assigned homework, that homework should map onto your treatment plan and the modality you’re supposedly using.
Core Categories of Therapeutic Worksheets
Cognitive Behavioral Therapy Tools
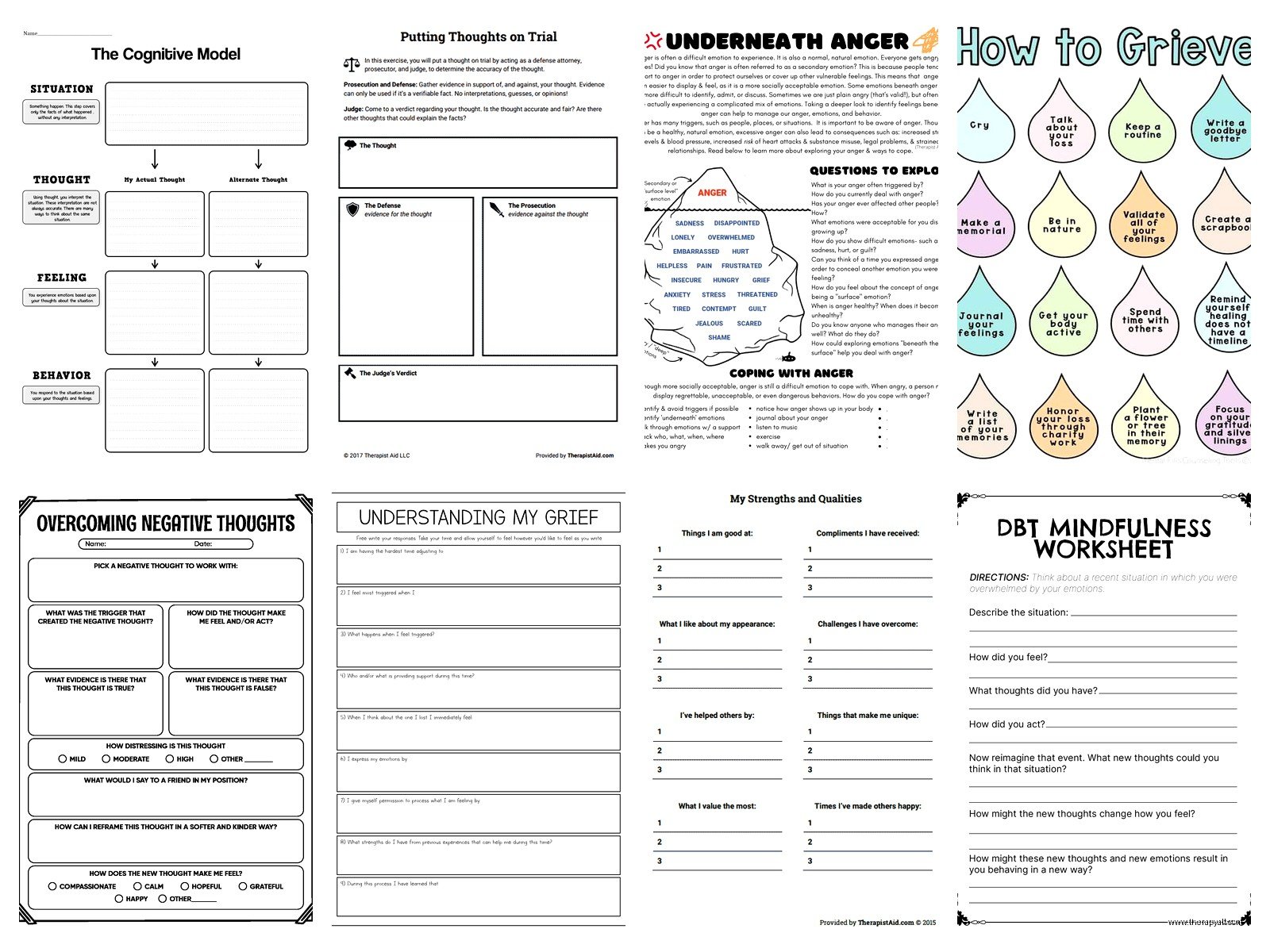
CBT worksheets are probably the most common and include thought records, behavioral activation schedules, exposure hierarchies, and cognitive distortion identification sheets. The classic thought record—situation, automatic thought, emotion, evidence for/against, alternative thought—is essentially a portable version of Socratic questioning. You’re teaching clients to examine their thinking patterns outside your office.
Behavioral activation worksheets track activities and mood ratings. They’re deceptively simple but genuinely effective for depression. You have clients schedule pleasurable or meaningful activities and rate their mood before and after. The data usually shows that doing things improves mood even when motivation is absent, which contradicts the depressive belief that “I need to feel better before I can do anything.”
Exposure hierarchies help with anxiety disorders. You list feared situations from least to most anxiety-provoking, assign SUDS ratings (subjective units of distress, usually 0-100), and work through them systematically. I’ve created probably fifty of these with clients who have specific phobias, social anxiety, OCD—they’re incredibly versatile.
Dialectical Behavior Therapy Worksheets
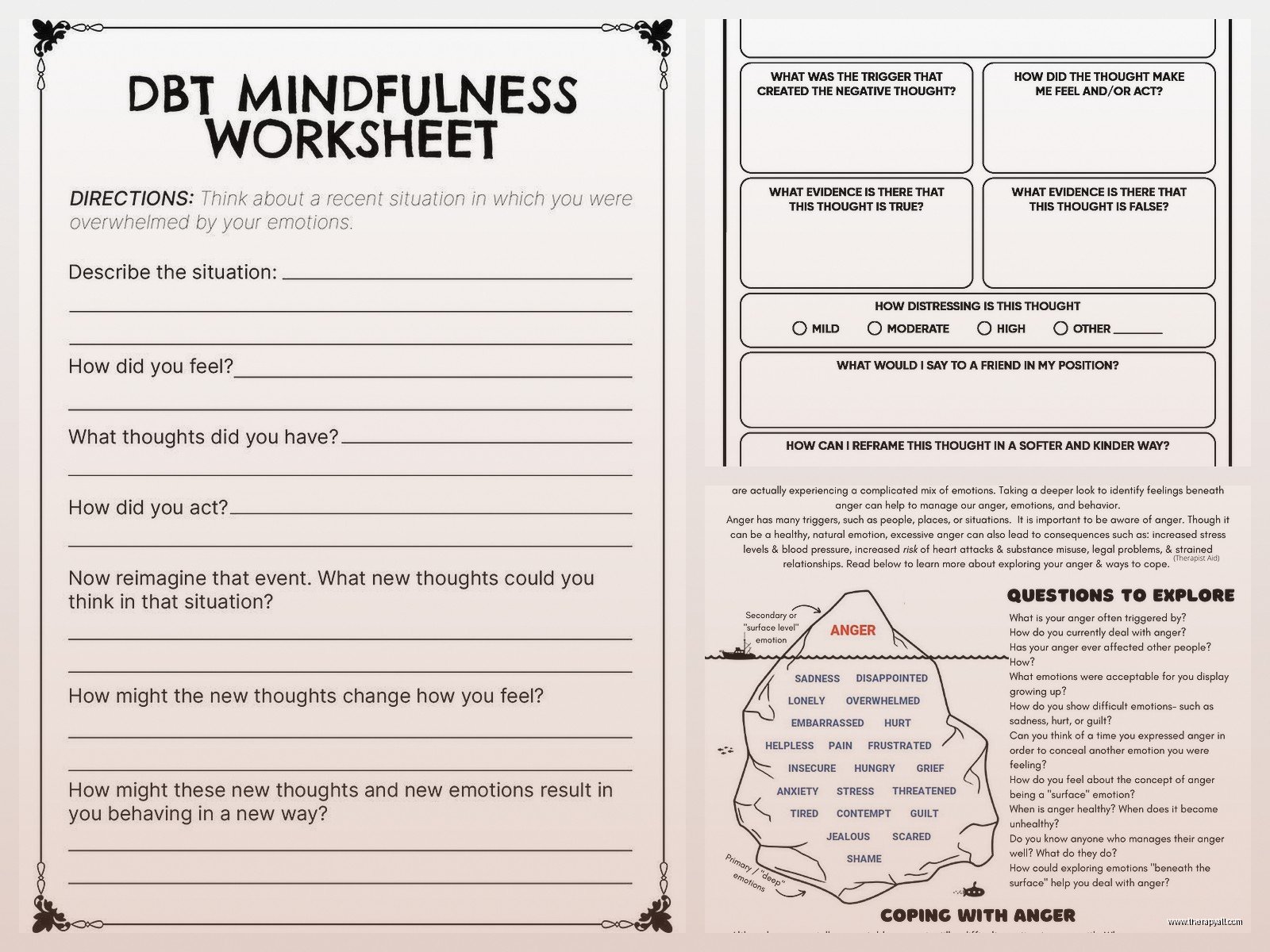
DBT has four skill modules: mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness. Each module has corresponding worksheets. The diary card is fundamental—clients track emotions, urges, skills used, and target behaviors daily. It sounds tedious and it kinda is, but it creates the data you need to identify patterns.
Distress tolerance worksheets often focus on the TIPP skill (Temperature, Intense exercise, Paced breathing, Paired muscle relaxation) or distraction techniques using the ACCEPTS acronym. I’ve had clients keep these in their phones as screenshots because when you’re in crisis, you’re not gonna remember seven different coping strategies without a prompt.
The emotion regulation worksheets include the ABC PLEASE skills (Accumulate positive emotions, Build mastery, Cope ahead, and the PLEASE skills for physical health). There’s also opposite action worksheets where you identify the emotion, the action urge, and then plan an opposite behavior. These work surprisingly well for anger and anxiety.
Acceptance and Commitment Therapy Materials
ACT worksheets focus on psychological flexibility, values clarification, defusion techniques, and committed action. Values worksheets ask clients to identify what matters most across life domains—relationships, work, health, leisure—and then assess whether their behavior aligns with those values. The discrepancy creates motivation for change without shame.
Defusion exercises help clients create distance from unhelpful thoughts. Worksheets might have clients write a difficult thought, then rewrite it as “I’m having the thought that…” or assign the thought to a character voice. My cat knocked over my coffee this morning and I immediately thought “I’m such a mess,” then caught myself doing the defusion thing automatically, which was weird.
Trauma-Focused Tools
Trauma processing worksheets need to be used carefully and only within appropriate therapeutic relationships. They include trauma narratives, stuck point logs (for CPT), and grounding technique reminders. The stuck point log identifies thoughts that keep clients from recovering—like “it was my fault” or “I should have fought back”—and these become targets for processing.
Grounding worksheets list sensory-based techniques (5-4-3-2-1 exercise, holding ice, describing objects in detail) that interrupt dissociation or flashbacks. You want clients to have these accessible during distress, not buried in a filing system at home.
Design Elements That Actually Matter
Worksheets need enough structure to guide but enough space to personalize. I’ve seen worksheets so cluttered with instructions and boxes that clients give up before starting. White space is your friend. Clear headers, numbered steps, and reasonable amounts of writing space make the difference between a tool that gets used and one that gets shoved in a bag.
Font size matters more than people think, especially if you work with older adults or clients with visual processing issues. Minimum 12-point font, preferably 14. Sans-serif fonts (Arial, Calibri) are easier to read than serif fonts for most people.
One thing that genuinely irritates me is worksheets that assume everyone has the same family structure, cultural background, or life circumstances. I’ve seen “family tree” worksheets that have zero flexibility for adoption, foster care, estrangement, or chosen family. Or couples worksheets that assume heterosexual relationships. It’s 2024—do better.
Digital Versus Paper Formats
This is more contentious than you’d think. Some therapists swear by paper because there’s something about writing by hand that aids processing and memory. Research somewhat supports this—handwriting activates different neural pathways than typing. But digital worksheets are searchable, don’t get lost, can include interactive elements, and are more accessible for clients with certain disabilities.
I personally provide both options. PDFs that clients can print or fill out on tablets, plus paper copies in session. Younger clients almost always prefer digital. Older clients are split—some love the convenience of digital, others find it alienating or… wait, I should mention that fillable PDFs need to actually work properly, which is a technical issue that’s caused me more headaches than I can count.
Therapy apps have built-in worksheet libraries now, which solves the organization problem but creates a dependency on specific platforms. If you switch EMR systems, you might lose access to your worksheet collection. Keep backups.
Customization and Adaptation
Pre-made worksheets are starting points. You’re gonna need to modify them for client reading level, cultural context, specific symptoms, and individual goals. A thought record for someone with OCD looks different than one for someone with PTSD—the types of thoughts and appropriate challenges differ.
Cultural adaptation is critical. A worksheet about assertiveness might need completely different examples depending on whether your client comes from an individualistic or collectivistic cultural background. Direct confrontation isn’t universally valued or safe.
I keep template versions that I modify in session with clients. We’ll go through a worksheet together first, I’ll point out what they can change or skip, and sometimes we’ll add sections. This collaborative approach increases buy-in and makes the worksheet actually relevant instead of generic.
Common Implementation Mistakes
Assigning worksheets without adequate explanation is probably the biggest error. Clients need to understand why they’re doing this, how it connects to their goals, and what to do if they get stuck. Just handing someone a thought record and saying “fill this out” is lazy therapy.
Over-assigning is another problem. Three worksheets per week is too many for most clients. They have lives, jobs, families, and limited cognitive resources. One well-chosen worksheet that actually gets completed is worth more than five that sit untouched.
Never assigning worksheets because you think they’re “not deep enough” or “too structured” is the opposite problem. Some therapists believe real therapy only happens in the room through conversation. But between-session practice is how skills generalize to real life. You can’t learn distress tolerance by talking about distress tolerance for fifty minutes weekly.
Not reviewing completed worksheets in session is surprisingly common and completely defeats the purpose. If clients take time to complete homework, you need to take time to discuss it, identify patterns, troubleshoot problems, and reinforce effort. Otherwise they’ll stop doing them, and rightfully so.
Where to Find Quality Worksheets
Therapist Aid is probably the most popular free resource—clean design, organized by topic and disorder, available in multiple languages. They have both free and paid membership options. The free worksheets are genuinely useful, not just teasers for paid content.
Psychology Tools offers high-quality CBT resources, though most require a subscription. Their worksheets include detailed therapist guides explaining the rationale and implementation, which is helpful for newer clinicians or when using a technique outside your primary training.
DBT Skills Training Handouts and Worksheets by Marsha Linehan is the authoritative source for DBT materials. Yes, you’re supposed to buy the book, not photocopy your colleague’s copy or download PDFs from random websites. Copyright matters, and also Linehan’s work deserves compensation.
ACT-specific resources come from Russ Harris’s books and the Association for Contextual Behavioral Science website. Steven Hayes’s books also include appendices with worksheets, though they tend to be more conceptual than practical.
Many therapists create their own, which is fine if you understand the underlying theory and treatment protocol. I’ve developed probably twenty custom worksheets over the years for specific client populations I work with frequently. Summer 2022 I was writing like three worksheet roundups a week for a mental health platform and started actually using them myself, which gave me a weird meta-awareness of whether instructions made sense.
Documentation and Clinical Records
You need to document worksheet assignments in progress notes and treatment plans. “Assigned CBT thought record to practice cognitive restructuring between sessions” is appropriate documentation. Keeping copies of completed worksheets in the clinical record is debatable—some therapists do, some don’t. It depends on your documentation philosophy and how the worksheets function in treatment.
If worksheets contain detailed trauma content or information that could be harmful if accessed by others, you need to consider carefully whether they belong in the official record or if summarizing the content is more appropriate. HIPAA doesn’t require you to include every piece of paper a client writes on.
Effectiveness Research
Homework compliance in therapy correlates with better outcomes across multiple studies. Clients who complete between-session assignments show greater symptom reduction and skill acquisition than those who don’t. The worksheets themselves aren’t magic—it’s the practice and repetition they facilitate.
But compliance rates are often low, ranging from 20-50% depending on the study and population. This isn’t necessarily client resistance. It’s often poor assignment selection, inadequate explanation, life chaos, or cognitive overload. If your clients consistently don’t complete worksheets, that’s clinical information about barriers that need addressing.
Some research suggests that reviewing worksheets in session matters more than just completing them. The therapeutic conversation about what clients noticed, where they struggled, and how to apply insights is where change happens. The worksheet is the vehicle, not the destination.